Heartfelt Thanks to MRC-Holland!
A heartfelt thank you to our generous donor, MRC-Holland, for your unwavering support!
Heartfelt Thanks to MRC-Holland! Read More »
A heartfelt thank you to our generous donor, MRC-Holland, for your unwavering support!
Heartfelt Thanks to MRC-Holland! Read More »
Happy Holidays and a wonderful New Year 2024! #Christmas2024 #NewYearGreetings #CommunityCelebration
Wishing the People to People community a joyous Christmas and a Happy New Year! Read More »
People to People Attains Not-for-Profit Status, Paving the Way for Transformative Impact in Higher Education, Healthcare, Youth, and Women’s Development Thompson Station, Tennessee – November 10, 2023

Vienna, VA – On October 21st, 2023, the P2P community came together to celebrate outstanding individuals. The P2P Awards recognized exemplary contributions in various categories: 🌟 Rising Star Award: Presented to Dr. Petros Wolde-Giorgis. 🤝 Community Service Award: Acknowledging the tireless efforts of Professor Panos Hatziandreas. 🌼 Lifetime Achievement Award: Conferred upon Professor Tilahun Yilma. 🏅 Congressional Medal Award: Bestowed upon Dr. Abera Molla. 🕊️ Posthumous Award: In memory of Dr. Adey Tsegaye Gebremedhin. 🔬 Leaders in Science & Technology: Recognizing the remarkable achievements of Professor Sossina Haile. 🙌 P2P Volunteer of the Year Award: Presented to Adey Hailu, MSc., Their contributions are not only acknowledged but celebrated with the hope of inspiring others to follow in their footsteps. Congratulations to all the esteemed awardees! #p2paward #WomensHealth #Trailblazers #HealthcareLeaders #communityservice #volunteeroftheyear
🏆 2023 P2P Awards Recognize Outstanding Achievements Read More »
On October 21, 2023, the Vienna Community Hall, VA, USA was the stage for a groundbreaking event in the realm of women’s health. Under the compelling theme ” Empowering Women, Transforming Healthcare,” we delved into the essential role of preventive healthcare in reshaping women’s lives. Engaging conversations on “Medicine & Health Care During Peace and Conflict” unveiled the resilience and adaptability needed to provide healthcare solutions in challenging environments. The concept of a “Triangular Partnership” was embraced with fervor, as we explored the significance of collaborations and bridges in elevating women’s health worldwide. The event reached its zenith with the P2P 2023 Honorees Award Presentation. Guided by our distinguished Moderator, the conference was a hub of knowledge-sharing, dialogue, and empowerment. Our heartfelt thanks go out to everyone who played a part in this incredible success. Together, we are sculpting a brighter and healthier future for women across the globe. Stay tuned for more updates and continue the dialogue on women’s health and empowerment! #P2P2023#WomensHealth #PreventiveCare #HealthcareForAll #ViennaVA #EmpowerWomen #SuccessfulConference #CommunityEvent
P2P 2023 Conference: An Empowering Success! Read More »
Join Our Exclusive Webinar on October 21st! We are excited to announce our upcoming webinar titled “Empowering Women: The Focus of the Upcoming Health Care and Medical Education” happening on October 21, 2023. Date: October 21, 2023 Time: Saturday, 8:00 AM to 5:00 PM Don’t miss out on this opportunity to gain valuable knowledge and network with like-minded professionals. Registration is now open! Reserve your spot today: https://us06web.zoom.us/…/reg…/WN_vm9MmsRGSHOljzd6hTLcfQ Visit our website for more details: https://p2pbridge.org/ We look forward to your participation and a knowledge-filled session! #webinar#ProfessionalDevelopment#networking#MedEd#Ethiopia
Join Our Exclusive Webinar on October 21st! Read More »

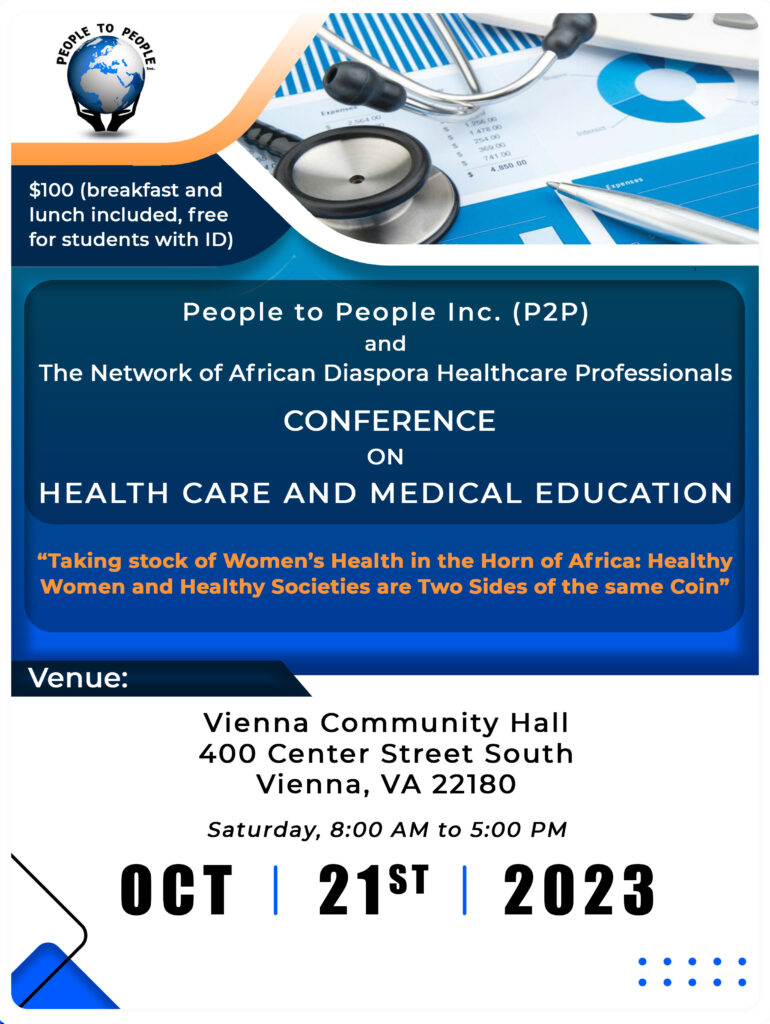
Theme: “*Taking stock of Women’s Health in the Horn of Africa: Healthy Women and Healthy Societies are Two Sides of the same Coin*” “Empowering women is empowering a nation.” Co-hosted by People to People Inc. (P2P) and The Network of African Diaspora Healthcare Professionals, this event is a must-attend! Register now https://www.paypal.com/donate/… Let’s unite to break barriers, foster inclusivity, and create change! Agenda Time Presentation (Topic) Speaker Allotted Time 8:00 AM – 8:30AM: Registration and Breakfast 8:30- 8:40 Welcome Enawgaw Mehari, MD P2P Founder & President 10 Minutes 8:40-8:50 Conference Logistics Kebede Begna, MD, MSc 10 Minutes 8:50-9:05 Opening Remarks H.E. Dr. Liya Tadesse Minister of Health, FDRE 15 minutes 9:05-9:30 Keynote: Healthy Women are the Cornerstones of a Healthy Society Senait Fisseha, MD, JD 25 minutes Session I: Prioritizing Preventive Services for Women: An Ounce of Prevention is Worth a Pound of Cure Moderators: Kebede Begna, MD and NURU ABSENO ROBI, MD 9:30-10:00 Breast Cancer Screening and Early Intervention Bethelhem Gelaw, MD 30 minutes 10:00-10:30 Cervical Cancer Screening and Prevention Wondimu Gudu Jeldu, MD 30 Minutes 10:30-11:00 Coffee/Tea Break 30 minutes 11:00-11:30 Obstetric Fistulae: Is the End in Sight? Rahel Nardos, MD, MSc 30 minutes 11:30-12:00 Infertility: The Landscape in Ethiopia Feruz Surur, MD 30 minutes 12:00 -12:30 Q&A/Panel Discussion All Speakers 30 minutes 12:30-13:30 Lunch Break 60 minutes Session II: Medicine & Health Care during peace and conflict Moderator: Demissie Alemayehu, PhD 13:30-13:40 Introduction: Health care impacts of conflict, role of the diaposra Demisse Alemyehu, PhD 10 minutes 13:40-14:00 War Inflicted Gender-Based Trauma & Mental Health; An Expert’s Perspective Yonas Geda, MD, MSc 20 minutes 14:00-14:30 Fostering Partnerships Ambassador Nora Dempsey. US Department of State 20 minutes 14:30-14:50 Q&A/Panel Discussion All Speakers 20 minutes Session III: Triangular Partnership; fostering partnerships and building bridges. Moderator: Anteneh Habte, MD 14:50-15:10 Accreditation of Universities & Medical Schools in Ethiopia; Status Update Lekidelu Taddesse-Heath, MD 20 minutes 15:10-15:30 Examplery works of the diaspora (walking the talk) Prof. Tilahun Yilma 20 minutes 15:30-16:00 Q&A/Panel Discussion All Speakers 30 minutes 16:00-16:30 Coffee/Tea Break 30 minutes Session IV: P2P 2023 Honorees Award Presentation Moderator: Ahmed Moen, PhD 16:30-17:00 Rising Star Dr. Petros Wolde-Giorgis Community Service Award Prof. Panos Hatziandreas Lifetime Achievement Prof. Tilahun Yilma Congressional Medal Dr. Abera Molla Posthumous Award Dr. Adey Tsegaye Gebremedhin Leaders in Science & Technology Professor Sossina Haile 17:00- 18:00 P2P Board Meeting
እንኳን ለደመራ እና ለብርሀነ መስቀሉ በሰላም አደረሳችሁ!
እንኳን ለደመራ እና ለብርሀነ መስቀሉ በሰላም አደረሳችሁ! Read More »

ለመላው የእስልምና እምነት ተከታዮች እንኳን ለመውሊድ በዓል አደረሳችሁ።
ለመላው የእስልምና እምነት ተከታዮች እንኳን ለመውሊድ በዓል አደረሳችሁ። Read More »
An Event Dedicated to Transforming Societies Through Women’s Health In a world where women’s health plays a pivotal role in the well-being of societies, a significant event is on the horizon. The “Conference on Health Care and Medical Education,” scheduled for October 21st, 2023, promises to shed light on a powerful truth: “Empowering women is empowering a nation.” For more details and registration information, visit the official conference website https://p2pbridge.org/